
In this final post, I examine the rationale behind the “do’s & don’ts” of diabetic health promotion, and provide resources for you to find out more about any pharmacotherapy your service users may be prescribed.
Health Promotion
When managing Type 2 diabetes (DM2), health promotion is arguably the most important of interventions: not only can it help to reduce the risk of the complications discussed in my previous post, but it could potentially lead to a remission. No drugs can do this. Admittedly, me talking about health promotion and its virtues is the easy part. Acting on it convincingly, passionately and consistently to service users and other healthcare colleagues; despite the food choices available on the High Street and in Hospitals; despite the very real and constant allure of substance use, junk food and a sedentary lifestyle… That’s the hard part.
The impact of various foodstuffs on the health of people with diabetes is a deeply complex issue. Most items of food we eat are likely to be a diverse mixture of macronutrients (fats, proteins and carbohydrates) and micronutrients (vitamins and minerals). In addition, any one of these components may be beneficial in one sense (e.g. glycaemic control), but a potential risk factor in another (e.g. atherosclerosis development). Over the last few years, there have been a number of proposed diets for people with DM2; When considering all potential health complications for people with DM2, there is no universally preferable diet (Dyson, 2014). NICE guidelines state that dietary advice should be individualised and given by healthcare professionals with specific expertise and competencies in nutrition. I’m no nutritional expert, but there are some aspects of health promotion that I feel comfortable discussing in this post.
First of all, there are a number of free resources that can support you and your service users:
- Practical diabetes: Diet and Weight Control: Extremely comprehensive and evidence-based blog posts around diabetes and nutritional advice.
- American Diabetes Association: Standards of Medical Care in Diabetes: Open-access journal supplement that details medical statements around diabetes management. It reads similarly to NICE Guidelines. Particular chapters of interest are 4 – Lifestyle management and 5 – Prevention or Delay of Type 2 Diabetes.
- Diabetes UK: Enjoy Food: Accessible and service user-facing set of resources that provides simple and practical advice.
- NHS: Type 2 Diabetes – Food and Keeping Active: Key aspects of general health promotion from the NHS.
Carbohydrates
 Sugary foods (simple carbohydrates) and refined carbohydrates such as white bread should be avoided. These foods cause blood sugars to rise dramatically and fall quickly. They are described as having a high Glycaemic Index (GI). Service users should aim to eat more wholemeal and high-fibre produce. These food sources take a time to be metabolised, so provide a steady and reasonable supply of glucose to the body over a number of hours. They have a low GI. There is a two-fold benefit here: Firstly, eating low GI carbs should mean that you can go longer between eating (reducing the temptation for snacking). Conversely, using high GI nutrients to repeatedly satiate hunger and low blood sugar levels can lead to a vicious cycle of unhealthy eating – to the point where the brain responds to these foodstuffs in a similar way to using addictive substances. Secondly, by relying on low GI carbs, there will be less dramatic rises and falls in blood glucose levels, making it easier to prevent dangerous episodes of hyper- or hypoglycaemia.
Sugary foods (simple carbohydrates) and refined carbohydrates such as white bread should be avoided. These foods cause blood sugars to rise dramatically and fall quickly. They are described as having a high Glycaemic Index (GI). Service users should aim to eat more wholemeal and high-fibre produce. These food sources take a time to be metabolised, so provide a steady and reasonable supply of glucose to the body over a number of hours. They have a low GI. There is a two-fold benefit here: Firstly, eating low GI carbs should mean that you can go longer between eating (reducing the temptation for snacking). Conversely, using high GI nutrients to repeatedly satiate hunger and low blood sugar levels can lead to a vicious cycle of unhealthy eating – to the point where the brain responds to these foodstuffs in a similar way to using addictive substances. Secondly, by relying on low GI carbs, there will be less dramatic rises and falls in blood glucose levels, making it easier to prevent dangerous episodes of hyper- or hypoglycaemia.
It’s unclear what the optimal amount of carbohydrate in a diet should be. Advice has ranged from 50% of a meal, down to minimal quantities of carb with ketogenic diets. For virtually any health outcome, clinical evidence hadn’t clearly favoured one over the other (Dyson, 2014)… that is, until a meta-analysis was released in the Lancet recently. This review brought together the findings of 185 prospective studies and concluded that at least 25g of daily dietary fibre is comprehensively good for us. It protects us from cardiovascular disease and type 2 diabetes, it helps to lower our cholesterol (see below), and can even reduce the chances of bowel and breast cancer. Dietary fibre can be best acquired through the consumption of whole-grain foods, which would necessitate the presence of a certain amount of carb in your diet.
Fats
 It may be worth knowing about the Glycaemic Index, but this only tells part of the story. For example, ice cream and chocolate gateau have relatively low GIs, but you wouldn’t be advocating their regular consumption to someone with diabetes. The main issue to consider with dietary fat content is the risk of cardiovascular disease (CVD). In my last post, I talked about LDLs (‘bad cholesterol’) and the associated risk of atherosclerosis. The question here is what causes our LDLs to rise? We tend to separate dietary fats into three broad categories: saturated fats, polyunsaturated fats and trans-fats. It can be beneficial for us to have a little fat in our diet, and polyunsaturated fats have the lowest associated risk of CVD. We find polyunsaturated fats in vegetable oil, nuts and fish. Trans-fats carry the greatest risk of CVD. Foodstuffs high in trans-fats (such as biscuits, cakes, ready-made pastries, beef-burgers and kebabs) should be avoided wherever possible. Saturated fats are more complicated: we need to be mindful of our saturated fat intake, as a diet high in red meat and dairy intake is likely to raise your LDLs. However, there are health benefits to some of the foods that contain saturated fat. For example, nutrients in low-fat dairy produce can actually improve aspects of blood glucose homeostasis.
It may be worth knowing about the Glycaemic Index, but this only tells part of the story. For example, ice cream and chocolate gateau have relatively low GIs, but you wouldn’t be advocating their regular consumption to someone with diabetes. The main issue to consider with dietary fat content is the risk of cardiovascular disease (CVD). In my last post, I talked about LDLs (‘bad cholesterol’) and the associated risk of atherosclerosis. The question here is what causes our LDLs to rise? We tend to separate dietary fats into three broad categories: saturated fats, polyunsaturated fats and trans-fats. It can be beneficial for us to have a little fat in our diet, and polyunsaturated fats have the lowest associated risk of CVD. We find polyunsaturated fats in vegetable oil, nuts and fish. Trans-fats carry the greatest risk of CVD. Foodstuffs high in trans-fats (such as biscuits, cakes, ready-made pastries, beef-burgers and kebabs) should be avoided wherever possible. Saturated fats are more complicated: we need to be mindful of our saturated fat intake, as a diet high in red meat and dairy intake is likely to raise your LDLs. However, there are health benefits to some of the foods that contain saturated fat. For example, nutrients in low-fat dairy produce can actually improve aspects of blood glucose homeostasis.
Other ways to fight diabetes and its health complications
Eating certain foods can reduce LDLs. In particular nuts, legumes (beans, peas and lentils), wholegrain cereals produce, and cocoa bean products. Yes – some chocolate could potentially help to lower cholesterol! However, it’s worth bearing in mind that most chocolate produce is high in sugar and saturated fat as well. Other lifestyle factors have been shown to increase LDLs: High caffeine intake, smoking, and high levels of stress.
People with diabetes also need to be mindful of their salt intake. High salt intake may not lead to increased LDLs, but it does cause the body to release antidiuretic hormone (ADH). ADH release causes thirst centre activation, increased water reabsorption in the nephron (this leads to raised blood volume when combined with increased fluid intake) and even vasoconstriction in high quantities. All of these changes lead to an increase in blood pressure, and hypertension is a risk factor for atherosclerosis and diabetic nephropathy development.
As with mental illness, there is a two-way relationship between sleep deficiency and DM2. Hyperglycaemia will lead to increased volumes of urine (see my last post for why this is), meaning more trips to the toilet during the night. There is a strong link between DM2 and obesity, and many people with obesity experience sleep apnoea – a condition can severely affect sleep quality. Sleep disruption itself has been linked to increased insulin resistance and weight gain. This can create something of a vicious cycle, but the opposite is true: if good sleep hygiene can be effectively managed, then this could contribute to the effective management of your service user’s DM2 as well.
Moderate Exercise
We all know that regular moderate exercise has certain health benefits; especially so for people with DM2, but what exactly are the effects of exercise on the body? The answer to this is staggeringly diverse:
- It assists in weight loss, aerobic fitness and muscle strength.
- Even without weight loss, it leads to improved insulin sensitivity and lowered HbA1c levels.
- It slows the decline of mobility in patients who are obese.
- In the long-term, it helps to reduce abdominal fat and blood pressure: particular risk factors for CVD.
- It reduces LDL levels and slows the rate of atherosclerosis development.
- It stabilises pre-existing atherosclerotic plaques and makes them less likely to rupture (which can lead to many different ischemic events).
- It improves mental health! It can alleviate the symptoms of a number of conditions, and in a number of different ways. For example, In depression, it can be as effective as CBT or antidepressant treatment.
- Both mental illnesses and diabetes are associated with a decrease in immune system function, but exercise can improve our immunity. There are a number of theories to why this may be.
National Guidelines state that we should all aim for at least 150 minutes of moderate exercise a week, or 75 minutes of vigorous exercise. These figures are mirrored by the Standards of Medical Care in Diabetes guidelines – for people with either DM1 or DM2. However, it is important to note that people who have been sedentary for long periods should ease into an exercise regime.
Non-Insulin Pharmacotherapies
While the pancreas continues to work, people with DM2 still produce insulin, even if it might not be in sufficient enough quantities for the body. There are a number of different medications that can aid the body with blood glucose homeostasis. These are of particular use when lifestyle promotion doesn’t have an effective enough impact. The number of drugs available seems to be growing exponentially, and there is a diverse range of ways these drugs affect the body – to the extent that this post would become unmanageably long if I discussed them all here. However, please bear in mind that because the drugs work in different ways, you may need to provide different pieces of accompanying advice, depending on the prescribed drug. Here are some links to websites where you can find out more about the drugs that your service user is on:
- Information for Service Users: Diabetes UK and Diabetes.co.uk
- BNF: Type 2 Diabetes Treatment Summary
- Medscape: Pharmacologic Therapy for DM2: This single webpage provides detailed information on all families of drugs used for DM2.
- General database for specific drugs: electronic Medicines Compendium (eMC): For detailed information on drugs, make sure you read the Summaries of Product Characteristics (SmPCs); for service user-facing info, look at the Patient Information Leaflets (PILs).
Different Types of Insulin
Although people may associate insulin use with Type 1 diabetes (DM1), individuals with DM2 will become insulin-dependent if the disease progresses far enough.
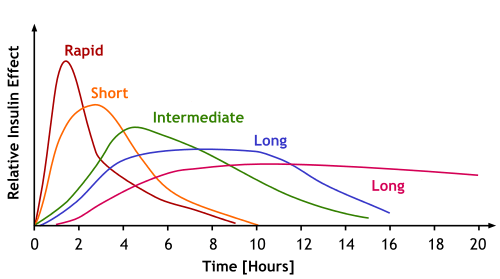
Speaking in general terms, insulin use tends to fall into one of two categories: those given after a meal to manage sudden increases in blood-glucose levels (postprandial or bolus doses), and those given to provide a steady effect throughout the day (basal doses). However, as the graph shows, there are many different patterns of effect – even between different long-acting insulins. Insulins can also come from a range of different forms and routes, as well as speeds. This page from Diabetes.co.uk provides a good level of information around different insulins. There is ample information on specific makes (e.g. Novorapid). If you help any service users administer insulin, then it may be worth reading around the types of insulin that they are prescribed here. Alternatively, this page from Diabetes UK provides plenty of good generalised info about insulin therapy.
Further Reading and References:
- Mulligan, K., McBain, H.B., Lamontagne-Godwin, F., Chapman, J., Flood, C., Haddad, M., Jones, J. & Simpson, A. 2018, Barriers to effective diabetes management – a survey of people with severe mental illness, BioMed Central.
- Department of Health: Improving the physical health of people with mental health problems: Actions for mental health nurses
- Dyson, P. (2014), Popular diets: are they effective for people with type 2 diabetes?. Pract Diab, 31: 187-192.
- Reynolds, A., Mann, J., Cummings, J., Winter, N., Mete, E. & Te Morenga, L. 2019, “Carbohydrate quality and human health: a series of systematic reviews and meta-analyses”, The Lancet, vol. 393, no. 10170, pp. 434-445.
- NICE Guidance: Type 2 diabetes in adults: management. Clinical Guideline Update (NG28). Methods, evidence and recommendations. December 2015 (unabridged pdf)
- NICE Guidance: Type 2 diabetes in adults: management (abridged web-based version)
- NICE Guidance: Physical activity: brief advice for adults in primary care
- Medscape: Type 2 Diabetes Mellitus. General US-based medical information hub.
- fit4diabetes.com: FIT Technique Plus. Insulin injection technique educational webpage.
Very good resources for nursing and student nurse. This will help us support our services users better.